|
I recently visited Monrovia, which in the words of P-Square, chopped my money. Food, accommodation, and transportation are much more expensive in Liberia than in any other West African country I have visited. It’s true that Liberia is a post-conflict country full of UN staff, who, when not struggling to help Liberia maintain its stability and get on its feet, are probably struggling to find enough things in Liberia to spend their money on. But Liberia also differs from other countries in West Africa in that the U.S. dollar is used in parallel to the Liberian dollar. Is it possible that dollarization could also contribute to higher prices? 
"Could we buy some dirt? That would help GDP, right?"
First, a couple of observations about money and prices in Liberia. The U.S. dollar and Liberian dollar are used interchangeably. There is no place that accepts only one. Generally, the U.S. dollars are used as large denomination bills, and the Liberian dollars are used in place of U.S. coins. (I didn’t see a single coin in Liberia.) Prices of imported goods in Liberian supermarkets are roughly the same as the dollar equivalent of prices of imported goods in Ghanaian supermarkets. Gas prices also seem to be similar, though a bit more expensive. It seems that the main difference in prices stems from differences in prices of services.
The fact that price differences are concentrated in services, or non-tradeables, makes me suspect that the high prices are in part due to dollarization, and here is why: in a non-dollarized economy, like Ghana, which uses the cedi, if the Ghanaian government pursues a loose monetary policy, the currency will depreciate relative to the U.S. dollar. This doesn’t affect the dollar price of imported goods—these are bought in dollars, so their price in Ghana cedis will just be inflated so that the equivalent price in dollars is unchanged. Other prices in the economy, however, are sticky. Employees have contracts with set wages, and people are used to paying a given price for hiring someone to sew a dress. As a result, the price of these non-tradeables stays constant in cedis, but becomes cheaper in dollar terms. (Note about monetary policy transmission in West Africa: In West Africa, business and consumer loans are much scarcer. So loosening monetary policy doesn’t lead to cheaper credit very quickly. It does, however, mean that cedi funds are more readily available to banks than U.S. dollar funds, which puts pressure on the exchange rate. So monetary policy transmission through exchange rates is more important in countries like Ghana, and happens more quickly, relative to transmission through interest rate mechanisms, compared to countries where large portions of the population have access to credit.) What this means is that Ghana, if has a trend of depreciating currency, can have low overall prices in dollar terms because, in dollar terms, prices for non-tradeables have fallen. Liberia, since it is dollarized, won’t see this effect. If Liberia prints more Liberian dollars, the exchange rate may change, with the value of the Liberian dollar declining, but prices in dollars will stay the same. This does, of course, attribute a level difference to an effect that applies to differences in rates of change, and my observations regarding prices of goods and services are anecdotal (Liberia doesn’t have good CPI data.) If you have comments on the plausibility of the theory, please comment!
5 Comments
Clearly, the nations of the world are not going to line up to let me randomize their monetary policy. But what if I could convince one to do so?
Randomized control trials (RCTs), when ethical and possible, present the most reliable way to measure the impact of policy. Units of randomization, for instance people, are put into a treatment group, who gets a program or policy, and a control group, that doesn't get the program or policy. You compare outcomes for the two groups to see the impact of the program. The key to the validity of the RCT is that the sample size has to be big enough that when you randomly divide into treatment and control, there are no important systemic differences between the two groups. Randomization isn't used to evaluate macroeconomic policies for 2 reasons: 1) it is usually too important for people to allow it to be randomized, and 2) it has to be enacted at a high level-- national or maybe state or province-- so it is difficult to get a large enough sample. But what if we randomized, not by entities like people or countries, but across years? For example, what if the Federal Reserve allowed me to randomly change the policy interest rate by +25 basis points, 0 basis points, or -25 basis points? Over a long enough time frame, the periods that fall into each randomization group should be statistically the same on average. This would allow us to look at the effect of the interest rate change on the economy. Of course, there are some kinks to be worked out. Similar to spillover effects, policy changes have impacts across multiple periods; however, these could be measured and accounted for. Another problem is checking the balance of the randomization. There would be no equivalent to a baseline, and you couldn't stratify, since you don't know the attributes of future time periods in advance. These problems would imply that you need a very large sample size. There are certainly other methodological challenges I haven't thought of. I imagine I will have plenty of time to think through them before the first problem-- the fact that politicians, who insist they can control things they can't, would never randomize something they can-- is solved. But if anyone hears about a central bank looking for a monetary policy consultant, let me know. Not Ghanaians. Despite the fact that Obama is pretty much universally liked, Ghanaians don't really see themselves as having any real stake in the election. I asked five of my colleagues, all highly educated Ghanaians who could name both presidential contenders, if they cared who won. All five answered, a little hesitantly, "umm...not really." They didn't see any difference in the attention or assistance Africa received with Obama at the helm compared with Bush. What do the numbers say? Here is U.S. foreign assistance appropriations for Ghana from 2006 to 2012: 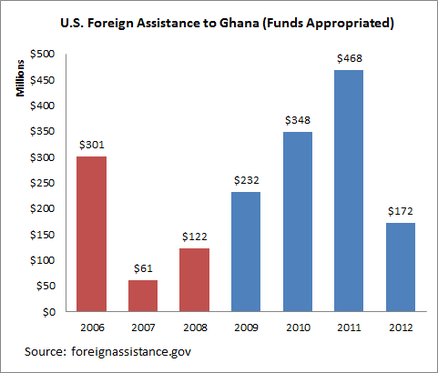 (foreignassistance.gov only gives data back to 2006, and I couldn't get the numbers to match up with Census Bureau data, which go back farther but are less current. If anyone knows how to reconcile the series, I'd love to show data for the whole Bush administration.)
Aid appears to be higher during the Obama administration. (The Census data suggest annual foreign aid of under $100 million a year for the earlier years of the Bush administration.) But wait-- how much of the Obama spending is actually the result of the MCC compact signed under Bush? Although MCC spending isn't trivial-- $457 million for the period-- USAID spending is still much higher, and over half of the MCC appropriations were in 2006. By my reading, Ghana was better off, in terms of simple U.S. dollar aid receipts, under Obama.  "A developed country is not a place where the poor have cars. It's where the rich use public transportation."
If the truth of this statement is not immediately apparent, you probably have never commuted in a West African city. Accra needs a lot of infrastructure improvements, but one thing it does not need are more cars. After work, I can run the two miles to my gym faster than I could take a taxi there. Traffic is similarly bad in Kumasi and Dakar, and is rapidly worsening in Tamale. Driving is no picnic in American cities, either. The difference? In American cities, rich people often choose to live in places accessible to public transportation, and their taxes and patronage support transit systems that benefit the rich and poor alike (even LA is getting on the bandwagon). In developing country cities, the poor take low quality public transit, such as trotros and shared taxis, while the rich clog the roads with their private cars and taxis. While roads in developing country cities could certainly be improved (I would love to see someone apply traffic light efficiency models to Accra traffic), the reality is there is limited capacity to expand current roads or build new ones in the middle of the city. Poor people are already taking public transport. That leaves one viable solution to traffic in developing country cities: getting rich people to convert to public transport. For practical and cultural reasons, this is an uphill battle. First, the main reason rich people use public transport in developed cities is not because they are altruistic, it is because it is faster and easier than driving. Accra currently has no public transit system that can rival the speed and efficiency of a private car. Considerable investment would have to be made in a rail or bus system with widespread coverage and efficiency in order to convince people to convert. Second, there is a cultural attachment to driving. Owning a car is a definitive status symbol in West Africa; taxi drivers are often confused when I, a person who apparently has the money to take a taxi, choose to walk. Improving traffic in Accra will require a commitment from the wealthy and elite-- both foreigners and Ghanaians-- to get out of their air conditioned Toyota Landcruisers and both fund and use public tran Last Saturday night around midnight, I was standing in the middle of a street in Tamale, trying in vain to beg or bribe a taxi driver to stop and take a dying man to the hospital. I hadn’t seen the motorcycle collision that injured this man and one other, but the small crowd, the battered bikes, and the bloody, limp bodies told the story clearly. My makeup, blond hair (combed for once), and red dress, which correctly marked me as a foreigner on my way to a dance club—normally very desirable fare for a taxi—suddenly carried little cachet. As multiple taxis turned me down, two of the man’s friends began a futile and possibly fatal attempt to load him onto the back of the motorcycle. His neck and limbs flopped sickeningly as the motorcycle sparked to life and died repeatedly.
In the end, the only way we could convince a driver to take the man to the hospital was to have a white person accompany him. A friend of mine drove ahead of the taxi on his own motorcycle, carrying one of the man’s friends. We paid the driver four times the going rate. As they drove away, a woman watching the scene remarked to me, “Of course the taxi driver can’t take the man. When he gets to the hospital, they will hold him responsible and make him pay if the man can’t.” Welcome to a world where individuals have the liberty not to have health coverage, and face the consequences for how they exercise that liberty. In Ghana, you don’t get treatment—sometimes even life-saving treatment—until you prove you can pay for it. Doctors will sit and watch you bleed while your friends and family cobble together money for payment, or rush to renew your health insurance policy. I once saw a four-year-old boy delivered to a rural health clinic after he ran onto the highway and was hit by a motorcycle. There was nothing the clinic could have done to save him. His mother spent his last moments not by his side, but running desperately through the village to get his insurance card. The issue of allowing indigent or liquidity-constrained individuals (those who could pay back their medical bills over time) to die aside, the serious economic issue here is that when the default assumption is that people cannot pay for health care, there are negative externalities that mean even those who can pay for care may not get it promptly, and as a result, may have worse outcomes. A man with thousands of cedis in his account should be able to get a taxi to the hospital; he should not be left on the road because the drivers fear he will be turned away on the hospital steps. A child with insurance should be treated promptly; he should not be left bleeding on a clinic table while his mother runs for proof of insurance. Those who support universal health care, or an insurance mandate, should not fail to recognize the costs, in terms of our government budget deficit, burden on the poor, and loss of economic freedom. However, those who are opposed to it should recognize the full costs of that liberty as well. The Three-Cups-of-Tea guy’s charity is getting sued, for allegedly misleading donors (posted on Chris Blattman and AidSpeak.) I agree it’s not a bad thing for NGOs to be held accountable for doing what they say they are going to do. However, I think this raises a very interesting point about whom NGOs are accountable to.
NGOs, like businesses, are accountable to their clients. Those of us who work where the rubber hits the road (assuming there is a road) probably like to think of the people who are the beneficiaries of our projects are our clients, and that the product we provide is improvement in their welfare. Time for a wake-up call. NGOs, like all economic entities, are, first and foremost, beholden to the people who give them money, and that means not beneficiaries, but donors. NGOs exist because a donor somewhere gets utility from a beneficiary getting a new school, or deworming, or ugly shoes, not because those people actually want them. The beneficiaries of our projects, and their welfare, are the product that we sell to donors. This isn’t a very flattering way to look at NGO work, but I think it’s a necessary one. There is potential for dissonance between what donors want people to have, what NGOs have an incentive to say they do, and what beneficiaries actually want and need, and this potential dissonance should be addressed, not ignored. This brings up the issue of research NGOs, like IPA. When viewed through this paradigm, research NGOs perhaps look the worst: the product that is being sold is not even beneficiary welfare itself, but data about beneficiary welfare. But this product is the key to addressing the problem of donor-NGO-beneficiary dissonance: donors who have good information about what actually helps people, and what NGOs are actually doing, what they demand from NGOs is more likely to align with the needs of beneficiaries. So maybe I can still feel pretty good about what I did today. Normal 0 false false false EN-US X-NONE X-NONE MicrosoftInternetExplorer4 /* Style Definitions */ table.MsoNormalTable {mso-style-name:"Table Normal"; mso-tstyle-rowband-size:0; mso-tstyle-colband-size:0; mso-style-noshow:yes; mso-style-priority:99; mso-style-qformat:yes; mso-style-parent:""; mso-padding-alt:0in 5.4pt 0in 5.4pt; mso-para-margin-top:0in; mso-para-margin-right:0in; mso-para-margin-bottom:10.0pt; mso-para-margin-left:0in; line-height:115%; mso-pagination:widow-orphan; font-size:11.0pt; font-family:"Calibri","sans-serif"; mso-ascii-font-family:Calibri; mso-ascii-theme-font:minor-latin; mso-fareast-font-family:"Times New Roman"; mso-fareast-theme-font:minor-fareast; mso-hansi-font-family:Calibri; mso-hansi-theme-font:minor-latin;} Looking at antenatal care stats for health facilities in Ghana always puts my problems into perspective (OMG my avocado is not ripe!!). Some highlights from the records I looked at today:
Birth years of women attending ANC: The oldest was born in 1970, the youngest in 1999. Educational attainment of women attending ANC: Most have no school; only one had been to high school. How women attending ANC got to the clinic: Women come by walking, tro tros, bicycle, riding on the back of motos, and canoe. In today’s data, the extreme athletics award goes to a woman, 8 months pregnant, who walked 180 minutes to get to the clinic. Americans in Ghana spend a lot of time being asked for stuff. Plenty of the things we are asked for are ridiculous (sums of money equal to half our monthly salaries, our hands in marriage). But honestly, we Americans, who worship individualism and self-sufficiency, aren't really the givey-receivey types anyway.
The fact is, the average Ghanaian is just as likely to give to an American generously as he or she is to ask for a generous gift. Unfortunately, Americans who only frequent ex-pat establishments often don't get to see this, as the ex-pat scene often attracts those people looking only for a rich source from which to ask. When you get out into Ghanaian communities, you see the other side of things. In my first week back from the states, I was given more things for free than I was asked for:
Receiving gifts can be more uncomfortable than being asked for them, especially when the person you are receiving the gift from appears to be poor compared with you. The things I have been offered have always been things that the giver could give without noticeably hurting their own well-being, even if the price I would have been willing to pay for the item would have improved it. The truly valuable thing I think I get from receiving gifts are lessons in being humble enough to accept a gift, open enough to permit the social tie the gift creates, and savvy enough to know when a gift is appropriate. Chris Blattman recently blogged about the moral absurdity of running regressions where the dependent variable is “war deaths”. While looking at death, illness, hunger, and poverty through the lens of statistics may seem rather reptilian, I think many researchers have emotional reactions to the data they work with. For me, these connections hit hard and unexpectedly, often when I am tired and working late, and they come despite efforts to be dispassionate about the data I am looking at.
Survey editing is prime territory for emotional connections to data. When editing surveys, you see the story of an individual respondent in a way that you don’t when you are looking at columns of aggregated data . Once, I was reading a survey where a respondent reported that a household member had experienced a headache. I turned the page to the question on outcomes of health events. The headache had resulted in death for that household member—despite the family spending an amount equal to roughly one-fourth of Ghana’s annual GDP per capita on health care for that individual. The shock of the outcome hit me almost physically. Another respondent reported testing positive for HIV. Sitting alone in the Tamale office at night, I struggled to pull myself together, shoo the bugs out of my computer keyboard, and make my way home. The “death” outcome became a dependent variable in regressions I later ran looking at determinants of health outcomes. Luckily, there were very few events of death in my sample. We also looked at a number of food insecurity events: individuals going to bed hungry, or not eating for an entire day, for example. These were, unfortunately, common among our respondents. I don’t deal well with feeling hungry myself, and for me, food insecurity statistics evoke desperately sad, human images: a man’s disappointment at foregoing his favorite fish; a young student trying to sleep before an exam while feeling the distracting ache of hunger; an elderly woman going without food for a day so her grandchildren can eat; a mother having to tell her thin children there is no food today. These emotional connections often seem like a distraction, something that prevents us from approaching our analysis logically and dispassionately. In all honesty, part of my attraction to quantitative research tools might be to protect myself from these types of emotional connections to problems. But it our ability to have these connections, even through layers of statistics, is tied to a very deep belief in the importance of what we are doing, and that counts for something. Hey, at least I’m not working in finance.  The pangolin, one of my favorite animals, recently made the news. This unusual looking anteater is being hunted to extinction due to demand for its meat and scales, which are believed to, among other things, enhance sexual prowess in traditional Asian medicine. Enforcement efforts have not been able to put a stop to the trade. Although trade in these products must continue to be illegal, and these laws must be enforced, they will not be sufficient to stem this problem. Here’s why: · Lesson from the drug war: fighting supply doesn’t work with products that have inelastic demand. When demand is not very price sensitive, limiting supply just causes the price of the product to rise, giving more incentive for people to keep supplying. Endangered species products for use in medicine likely fall into this category, as likely perceive these medical cures as a need. According to the article, an entire dead pangolin used to be valued at $5; today the scales alone go for $250. Powdered rhino horn can be more valuable by weight than gold or cocaine. That’s a pretty big incentive to break the law. · Economic conditions will continue to enable higher prices and more demand. Rising incomes in China and South East Asia, the source of much of the demand for endangered species products, will further accommodate higher prices for these products. · Creating efficient disincentives in the source countries is difficult. When deciding whether to break a law, economic actors compare the benefit of the crime with the penalty, weighted by the likelihood they will get caught. In poor countries, the resources available for enforcement are limited, so likelihood of getting caught can be low. Higher prices, driven by the previous two factors, can entice more sophisticated suppliers to enter the market, who are better at evading enforcement efforts. In cases where suppliers are poor, penalties such as fines may be ineffective, because the supplier has little to lose. · Endangered species parts might be non-normal goods—meaning that higher prices actually raise demand. In the case of medicines, a higher priced medicine might create a larger placebo effect, for the same reason people who know the price of an expensive wine tend to rate its taste more highly. In the case of luxury goods, the scarcity of the product, and fact that it is illicit, might actually increase the prestige associated with owning it. These factors imply that to put a real stop to endangered species products trade, we must address the demand side. There are a couple potential approaches:
1. Try to shift the demand curve left. This involves decreasing the number of people demanding the product, or decreasing the amount of product that each person demands. In order to do this, you have to convince people that they don’t need these products, or that they are inferior to other options. Intense education, shame campaigns, and social pressure to embrace modern medicines might be approaches to achieving this. 2. Make demand more elastic by increasing substitutes. If you cannot convince people they don’t need these products, you might still be able to make demand more price sensitive if you can convince them that other substitutes can suffice. Endangered species parts might be replaced with parts from more common animals in traditional medicine recipes. This might be achieved by working with practitioners of traditional medicine to promote recipes that don’t include endangered species parts. This strategy, however, runs the risk of transferring the over-demand to other species. Any strategy aimed at demand is incredibly daunting, as it involves changing long-held cultural beliefs and behaviors, practiced even among the highly educated. And some traditional medicines work: ma huang, traditionally used to treat colds, contains pseudoephedrine, the active ingredient in many over-the-counter cold medicines, and Artemisia, another traditional medicine, is now a standard component in most malaria treatments. It is not easy to convince people that while their age-old belief that Artemisia cures malaria is true, their age-old belief that anything remotely phallic increases sexual prowess isn’t. Though if you think a pangolin looks phallic, you are probably long overdue for an STD screening. |
About Liz
I have worked in economic policy and research in Washington, D.C. and Ghana. My husband and I recently moved to Guyana, where I am working for the Ministry of Finance. I like riding motorcycle, outdoor sports, foreign currencies, capybaras, and having opinions. Archives
December 2016
Categories
All
|
 RSS Feed
RSS Feed
